I have been behind on providing updates on my upper extremities recovery (arm and hand). I started writing this entry over 2 years ago. There’s a lot to share and I wanted to provide as much information as I can with what I’ve learned so far. A lot of this is a recap from beginning to almost current. I also think it has a lot to do with the lack ofimprovementI’m seeing. It is also so minor (in my mind) that I don’t feel I had anything worth sharing. However, looking back I remember having zero mobility from my shoulder down. My left arm hung there helplessly and I would have to pick it up with my right hand and ‘carry’ it with me.
Honestly, I miss using my left arm and hand so much. It pains me everyday to only use half of my body. I’ve made sacrifices and been limited to enjoy the things I love to do. I have gone through many valleys of depression because of this and I’m not where I want to be. However, I want to share encouragement and truth with those going through a similar trial because I understand your pain and loss. I keep reminding myself regardless of how I feel or how I may disregard my progress, I want to be truthful to my word and share what my progress has been thus far. I may not be where I want to be yet but I have put in a lot of work and more importantly 🙌🏼
ALL GLORY TO GOD!
“always giving thanks to God the Father for everything, in the name of our Lord Jesus Christ.”
Ephesians 5:20
You never realize how much you use your non-dominant side … until you can’t use it. For those who had a broken arm understand this temporary inconvenience. I pray that mine is temporary because living 2 years without the use of it where my biggest depression and fear lies. It does take 2 hands to tear toilet paper or a paper towel. Pulling up or buttoning your jeans / pants, looping your belt or putting up your hair in a ponytail. Even a basic need to rub or scratch an itch on my right side has been taken away from me. I’ve been having to use the corners of my wall to scratch my right arm. I cut off 9 inches of hair after my stroke because I couldn’t maintain it independently. The list does goes on and on and on and on…
Immediately after my stroke, my left arm felt as though it weighed a ton. For the first few days, I didn’t feel anything in my arm. After a week in ICU, I remember waking up one morning and my fingers started to have some strange movement. I was extremely excited at first until I realized it was done involuntary. I couldn’t reproduce the movement. Looking back this was the first time spasticity started.
I’ve explained spasticity before in prior posts. It’s the devil! The stroke damaged my neural pathway in my brain and now my brain doesn’t know how to control my muscles. It doesn’t know if my fingers should be flexed or relaxed. As the brain continues to misfire connections, spasticity occurs.
Spasticity is a condition in which there is an abnormal increase in muscle tone or stiffness of muscle, which might interfere with movement, speech, or be associated with discomfort or pain. Spasticity is usually caused by damage to nerve pathways within the brain or spinal cord that control muscle movement.
A big misconception is that a stroke causes damage to the muscle. That is incorrect. The muscles are totally fine. A stroke causes damage to the brain 🧠 and as a result of the brain damage, the neural pathways that send signals to the muscles are damaged. The longer the pathways are damaged, spasticity happens and the muscle gets weaker because there’s no input to move it.
My first day of outpatient rehabilitation was on August 3, 2021. I recall going into a side room to have my first OT evaluation. I was asked to shrug my shoulders up and back. Raise my arm, move my wrist, open my hand. All of which I failed. There was no visible movement on my left side. My therapist did make a comment and said I had “trace” movement in my shoulders.
Trace movement means there is visible or palpable contraction but no motion.
For the next few weeks I worked on “passive” ROM (Range of Motion) exercises. These were exercises where I passively moved my left arm with the assistance of my right arm. I would rock my left arm like a baby to give it input and get it moving. I would sit in front of a mirror and attempt to shrug my shoulders. I did these exercises several times a day trying to make the neural connections with my arm and hand to connect to my brain.
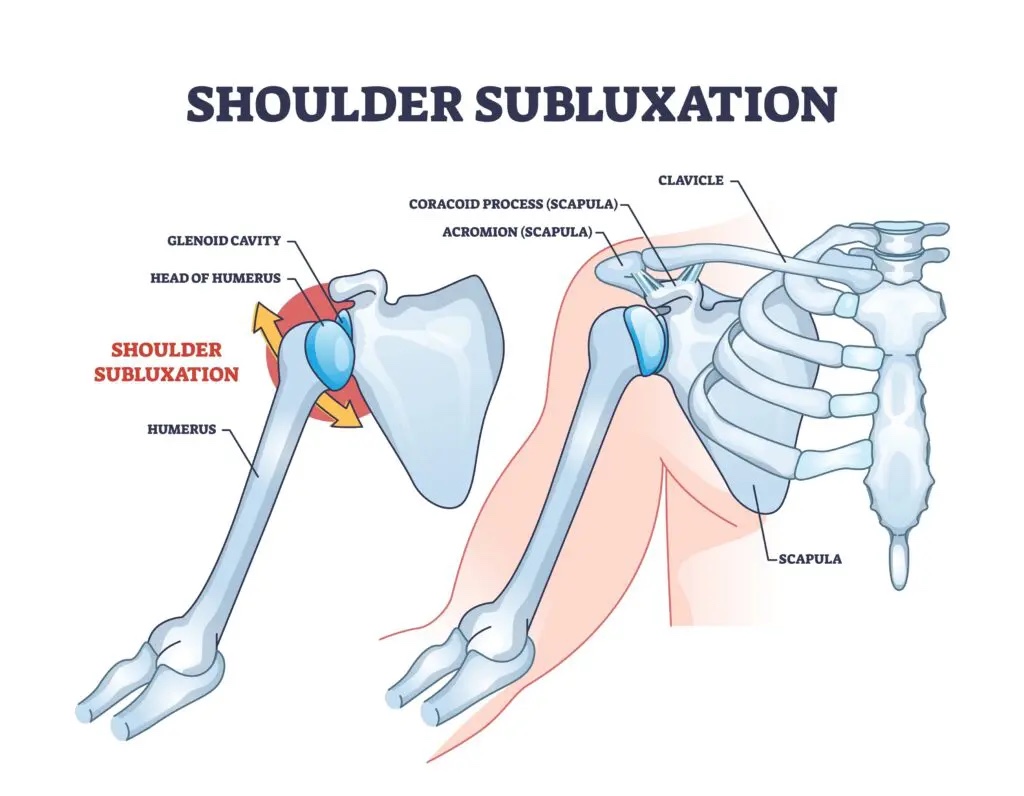
I ended up with a subluxation in my shoulder which is very common for those who had a stroke. Because the muscle around the rotator cuff in my shoulder is weak and as that muscle continued to weaken, the gravity pulling down from my left arm caused the humerus to “drop” lower in the socket. Anytime I was standing or learning how to walk, I had to wear a arm sling to ensure the drop didn’t continue to get worse. It was extremely uncomfortable and painful all hours of the day. I couldn’t sleep at night because of the pain. I would pray through the pain because I didn’t want to be drugged up, I needed to awake to put in the work. This lasted for about 4 months. If I moved in bed, I had to remember to be careful and ‘bring’ my arm with me because it was common to accidentally leave it behind. I mainly slept in one position (on my back) to avoid accidentally causing more pain.
My shoulder subluxation was a huge set back in my recovery journey . There’s no operation for a sublaxed shoulder because nothing is broken. My muscles needed time to repair themselves and get stronger to “hold” my humerus in place. That just BLOWS my mind how God designed our body. My muscle needs to get strong enough to hold my bone in place AND ALL of this is controlled by my BRAIN. 🤯 My therapist’s main focus was strengthening my shoulder muscle naturally so I could get it strong enough to heal my subluxation and I could start other arm therapy. We worked on what I could without further injuring myself and my job was to push myself through the discomfort and pain.
Watch all videos with volume, my Occupational Therapist is wonderful at explaining what we are working on and queuing me to recruit the right muscles.
Gravity eliminated Arm Flexion 11/17/2021 147 days post stroke | 4 mo post stroke
These are all performed laying down to eliminate gravity. You can see in the above video how shaky and slow my arm is. We had been working on this for several weeks before I could get a video clip. To even get this far, we worked our way up baby steps to where she would passively raise my arm and my only job was to feel the movement. I wish I had videos of where my arm totally smacked me in the face because that did happen a few times! My therapist kept telling me to focus on form and not speed. Speed will come but it’s important to rebuild those neural pathways first. All movement is good input to the brain. I remember I still had a subluxation in this video but I could still put in the work to strengthen my muscle .
Remember it is repetition, repetition, repetition! So those of you going through this, DO NOT GIVE UP! It is a lot of work but you can make it happen!
Arm Flexion with 3lb weight 7/1/2022 373 days post stroke | 12 mo post stroke
Everyone is different in their recovery journey. My recovery of movement seemed to start from shoulder down to my elbow to wrist. They say fingers and toes are the last to come back and now being 2 years out, I have yet to gain full functional mobility. Your stroke may have impacted you in a different way.
It’s difficult to compare leg recovery to arm recovery. When most people ask ‘Can you walk?’, they are asking if you can get from point A to point B. However, asking that same question ‘Can you move your arm?’ is different. Arm movement doesn’t equate to functional movement the same way you think for walking. There are so many facets and neural pathways that need to recover to make your arm perform a simple, functional task. Listed below is just a few of them that we work on strengthening in therapy:
Scapula
Shoulder
Tricep
Bicep
Supination
Pronation
Wrist flexion
Wrist extension
Finger(s) extension
Finger(s) flexion
Thumb abduction and thumb adduction
Lats – latissimus dorsi muscle
Pecs – pectoralis muscle
Deltoid (anterior, lateral and posterior)
Rhomboids (major & minor)
I share this with you because the journey to arm recovery takes a lot of work and TIME. This is why you may see most survivors start to make more gains in lower extremities compared to upper extremities. I don’t have a degree in anatomy. I’m learning real time in my journey and passing on what I’m learning to you. I’ve only learned this by trying to figure out what I need to do to get my arm and hand to start functioning again. Every time I failed to make a movement like turn on a light switch, I would ask my therapist why it was so difficult and she tell me to be patient because trying to perform a functional arm movement is not the same as learning to walk again.
I’m going to give you Stephanie’s best explanation of what is involved to do a simple task, such as turning on a light switch:
Biceps need to contract, as I engage my shoulder to extend my arm out (simultaneously my scapula needs to rotate upward) my biceps release as my triceps extend my forearm forward 90 degrees in front of me, while pronating forearm and engaging wrist extension, then extending just my index finger to push the light switch.
All that being said, combined movements are difficult after a stroke. While my brain is learning how to do one thing, it has to maintain the strength to hold the muscle and send signals to another muscle to perform a different task while still performing the previous task. The more combined movements, the more endurance is needed (hence why we strengthen muscles) and the brain works to fire signals. Additionally, muscles need to learn to work together. As an example, biceps need to engage when needed but also disengage when triceps are needed (muscle co-contraction) . Each has a different role to play. Pre-stroke our brain is firing this in nanoseconds but after a stroke, that connection needs to be rebuilt and that’s where repetition comes in. The more repetitive the motion, the more that pathway gets fortified through a new detour in the brain.
4 months after my stroke, due to my subluxation, I’m just learning how to do arm flexion laying down. So there’s a billion other things that I need to relearn. Keep in mind after a stroke, the nerve signals I had to do all these movements were damaged so I have quite a ways to go.
It is important for anyone who had a stroke or any TBI to continue therapy. An hour of therapy is not enough so you must do what you can at home.
In the hour of Occupational therapy at the clinic, we work on regaining movement in my shoulder, strengthening triceps and learning how to incorporate the use of my scapula again.
Strengthening the scapula is incredibly important for arm movement. Because the severity of my stroke, without strengthening the scapula muscle, I was limiting my mobility and using compensatory movement. This was something my therapist and I noticed right away. I wanted to put a stop to it so I asked to work on functional movement without using compensatory movement.
Compensatory movements usually occur in stroke survivors with hemiplegia, which is detrimental to recovery.
I just wanted to use the right muscles to perform a task. I didn’t want to hike my shoulder when I went to move my arm. I shared with my therapist that my recovery goal was to relearn my functional movements the way my body was designed to operate, pre- stroke – using all appropriate muscles to perform the task. I will tell you firsthand, this is not an easy task. There are many setbacks and frustrations. It has taken me double the effort and probably why my arm recovering has taken so long. But this is the recovery journey path I have chosen which may not be the same for you. I didn’t want to teach my brain how to do things the incorrect way and have to unlearn them to do it the correct way. Learning it once the right way was my goal.
An example of a compensatory movement is moving your torsoforward to reach and turn on the facet. (In some cases that may be needed if you are further away than normal distance but this example is within normal distance) Normal movement would be to learn to protract your scapula and extend your arm further to turn on the faucet without moving your torso. This is how you would’ve done it pre-stroke. Both actions have the same outcome. My personal goal is fight as much as possible to be back to pre-stroke me.
I will not let some doctor write my story. I will not be another textbook statistic that say those who had a stroke will never be the same.
I believe the brain is powerful, it has the ability to continuously learn and grow. I serve a loving Father who has given me a fighting spirit and furthermore He is the greatest physician. I will commit to put in the work and trust Jesus to continue writing my story.
The scapula engages in 6 types of motion, which allow for full-functional upper extremity movement including protraction, retraction, elevation, depression, upward rotation, and downward rotation.
Watch all videos with volume, my Occupational Therapist is wonderful at explaining what we are working on and queuing me to recruit the right muscles.
Scapular exercise using door frame for good posture (to keep shoulder from pulling in) 12/20/22 | 17 mo post strokeScapular exercise using door frame for good posture (to keep shoulder from pulling in) 12/20/22 | 17 mo post strokeStanding Scapula exercise with elbow splint (used to keep elbow straight) 5/3/2023 | 22 mo post strokeGravity eliminated Scapula exercise with elbow splint (used to keep elbow straight) 5/3/2023 | 22 mo post stroke
Please reach out if you have questions on arm mobility. I’ll continue to share more recent updates and my finger movement as they start waking up. 🙌🏼 Even if you are 6 month post stroke – CONTINUE TO FIGHT TO REBUILD THOSE NEURAL PATHWAYS. BE PATIENT WITH YOURSELF AND DO NOT GIVE UP!